Are they awake and breathing?
No normal breathing, gasping, no pulse, or gray-blue color should be treated as cardiac arrest until proven otherwise.
Patient guide + clinician detail
Collapse is a description, not a diagnosis. A person may faint, seize, suffer cardiac arrest, lose blood pressure, have low blood sugar, develop stroke symptoms, become overheated, or be overwhelmed by infection, toxins, trauma, or shock.
First principle
People use the word collapse for many different events. Some are brief fainting episodes with quick recovery. Others are life-threatening emergencies where the heart stops, breathing is abnormal, blood pressure falls, the brain is injured, or the body cannot deliver enough oxygen and sugar to vital organs.
The details around the event matter: what the person was doing, warning symptoms, pulse and breathing, color, movements, injuries, medicines, diabetes history, pregnancy, fever, bleeding, dehydration, and how quickly they recovered.
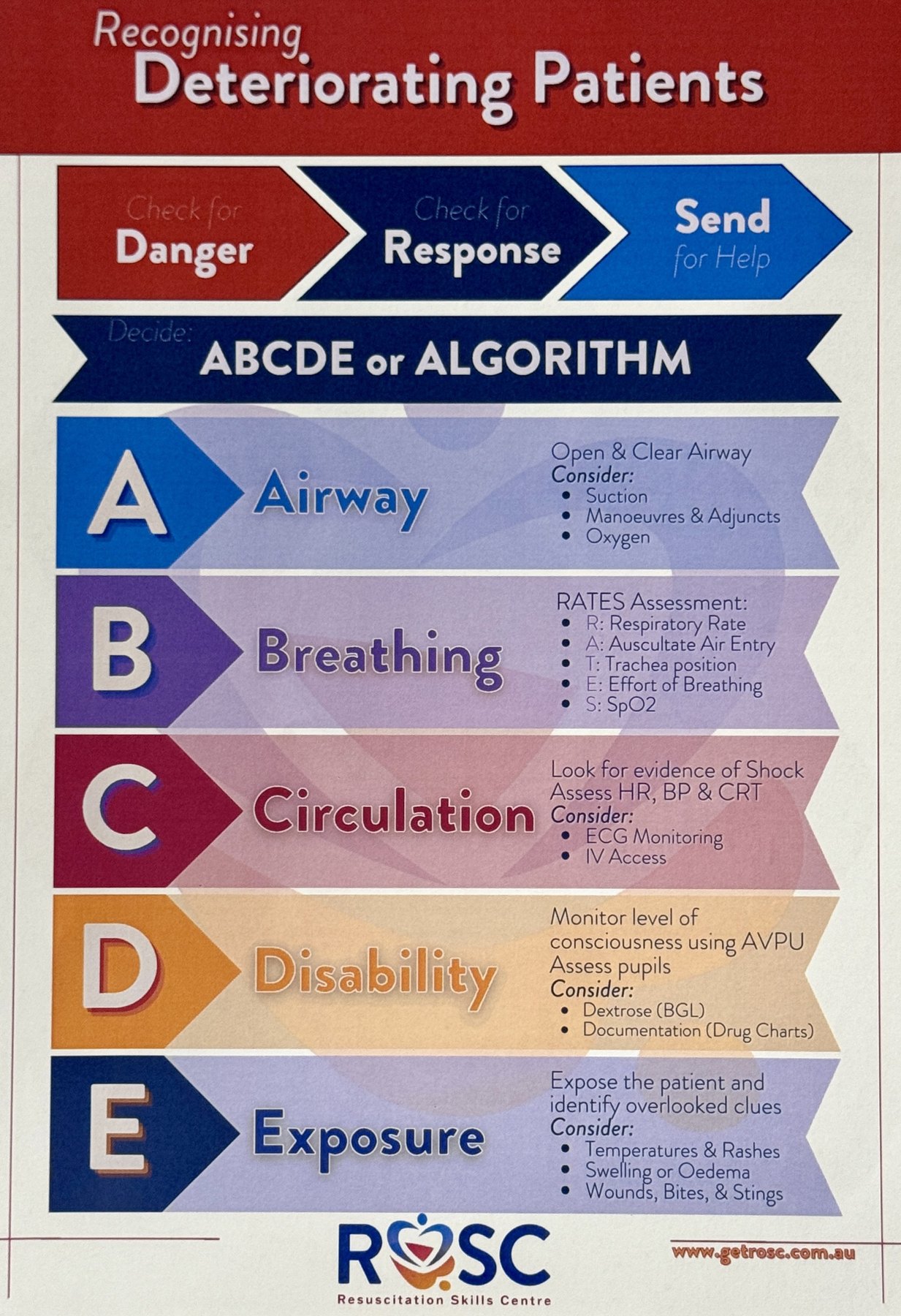
Collapse should be framed by physiology and tempo: transient loss of consciousness, syncope, seizure, cardiac arrest, shock, mechanical fall, intoxication, acute neurologic deficit, metabolic encephalopathy, or psychogenic nonepileptic event. Immediate priorities are responsiveness, airway, breathing, pulse, trauma, glucose, ECG rhythm, oxygen saturation, temperature, and hemorrhage control.
After stabilization, sort by pre-event context, prodrome, posture, exertion, palpitations, chest pain, dyspnea, focal neurologic signs, witnessed motor activity, tongue biting, incontinence, post-event confusion, medication exposures, substance use, pregnancy risk, and recurrence pattern.
Pattern recognition
No normal breathing, gasping, no pulse, or gray-blue color should be treated as cardiac arrest until proven otherwise.
Nausea, warmth, sweating, tunnel vision, pain, standing, dehydration, or fear can fit fainting. Chest pain, palpitations, or exertion are higher-risk clues.
Stiffening, rhythmic jerking, head turn, cyanosis, injury, or prolonged unresponsiveness may point toward seizure or arrest, though fainting can also have brief jerks.
Rapid, clear recovery can fit simple syncope. Confusion, weakness, headache, chest symptoms, or repeated collapse deserves urgent evaluation.
Cause map
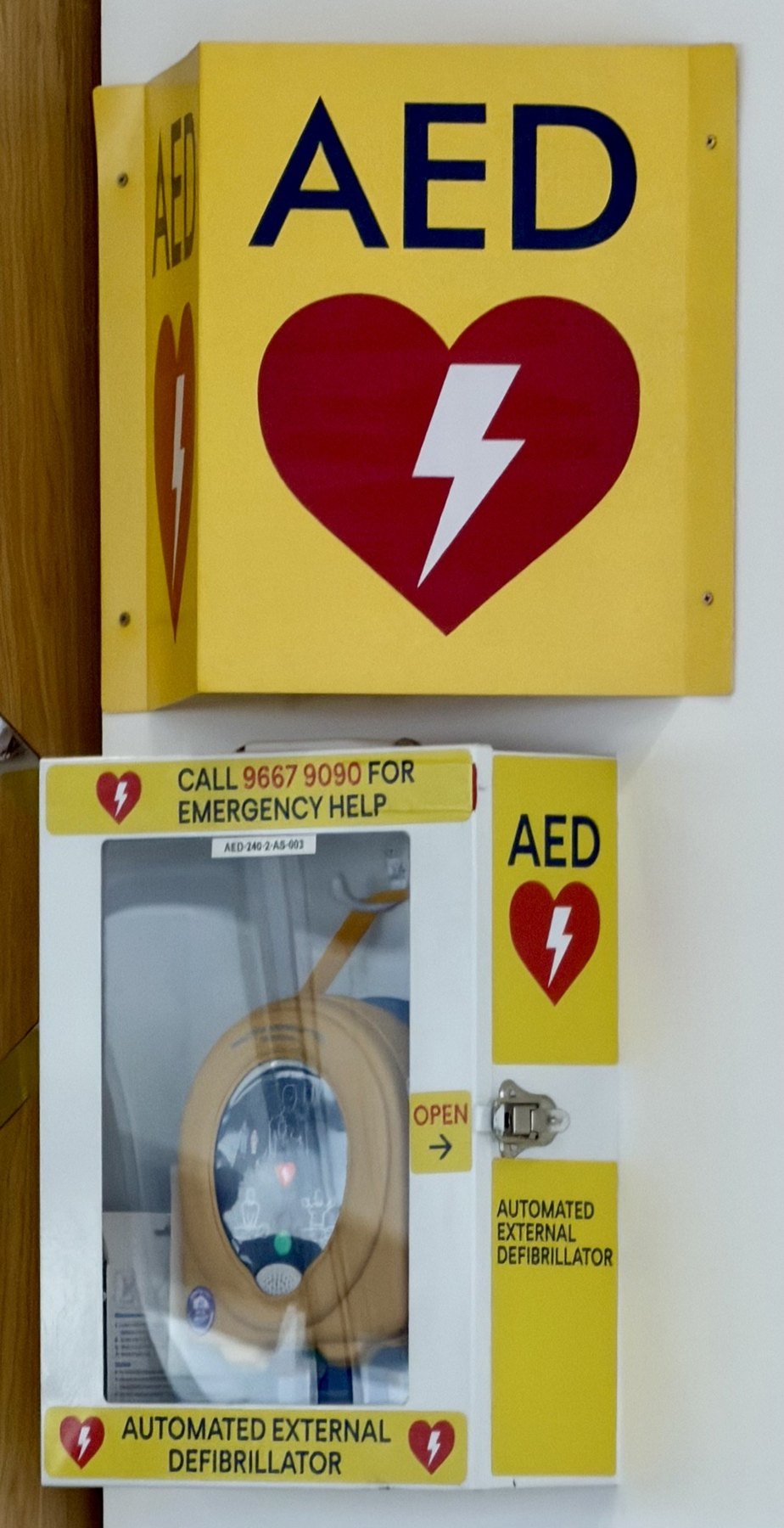
If the heart suddenly stops pumping effectively, a person may collapse without warning and stop breathing normally. Gasping is not normal breathing. CPR and an AED can be lifesaving.
Clue: sudden collapse during exercise, chest pain, palpitations, known heart disease, or a family history of sudden death raises concern.
Consider VT/VF, bradyarrhythmia, heart block, channelopathy, HCM, ARVC, ischemia, myocarditis, electrolyte disturbance, prolonged QT, Brugada pattern, drug toxicity, PE, tamponade, tension pneumothorax, hypoxia, and hemorrhage. Treat pulselessness first; refine etiology after ROSC or stabilization.
Syncope means a brief loss of consciousness from reduced blood flow to the brain. It may happen from standing, dehydration, pain, fear, heat, coughing, urinating, medicines, or a sudden blood pressure drop.
Clue: lightheadedness, sweating, nausea, warmth, ringing ears, or tunnel vision before collapsing can fit fainting.
Separate reflex syncope, orthostatic hypotension, medication-related hypotension, volume depletion, autonomic failure, situational syncope, carotid sinus syndrome, and cardiac syncope. High-risk features include exertional/supine events, structural heart disease, abnormal ECG, family sudden death, severe anemia, hypotension, dyspnea, and chest pain.
A seizure can cause sudden collapse, stiffening, shaking, staring, unusual movements, or loss of awareness. Afterward, the person may be confused, sleepy, sore, or have a headache.
Call for help: seizure lasting over 5 minutes, repeated seizures, trouble breathing, injury, first seizure, pregnancy, diabetes, or seizure in water needs emergency care.
Differentiate epileptic seizure, convulsive syncope, PNES, intoxication, hypoglycemia, hyponatremia, intracranial hemorrhage, infection, withdrawal, eclampsia, and trauma. Witness history, postictal state, lateral tongue bite, focal onset, prior epilepsy, medication adherence, and metabolic data are often more useful than routine imaging in clearly low-risk cases.
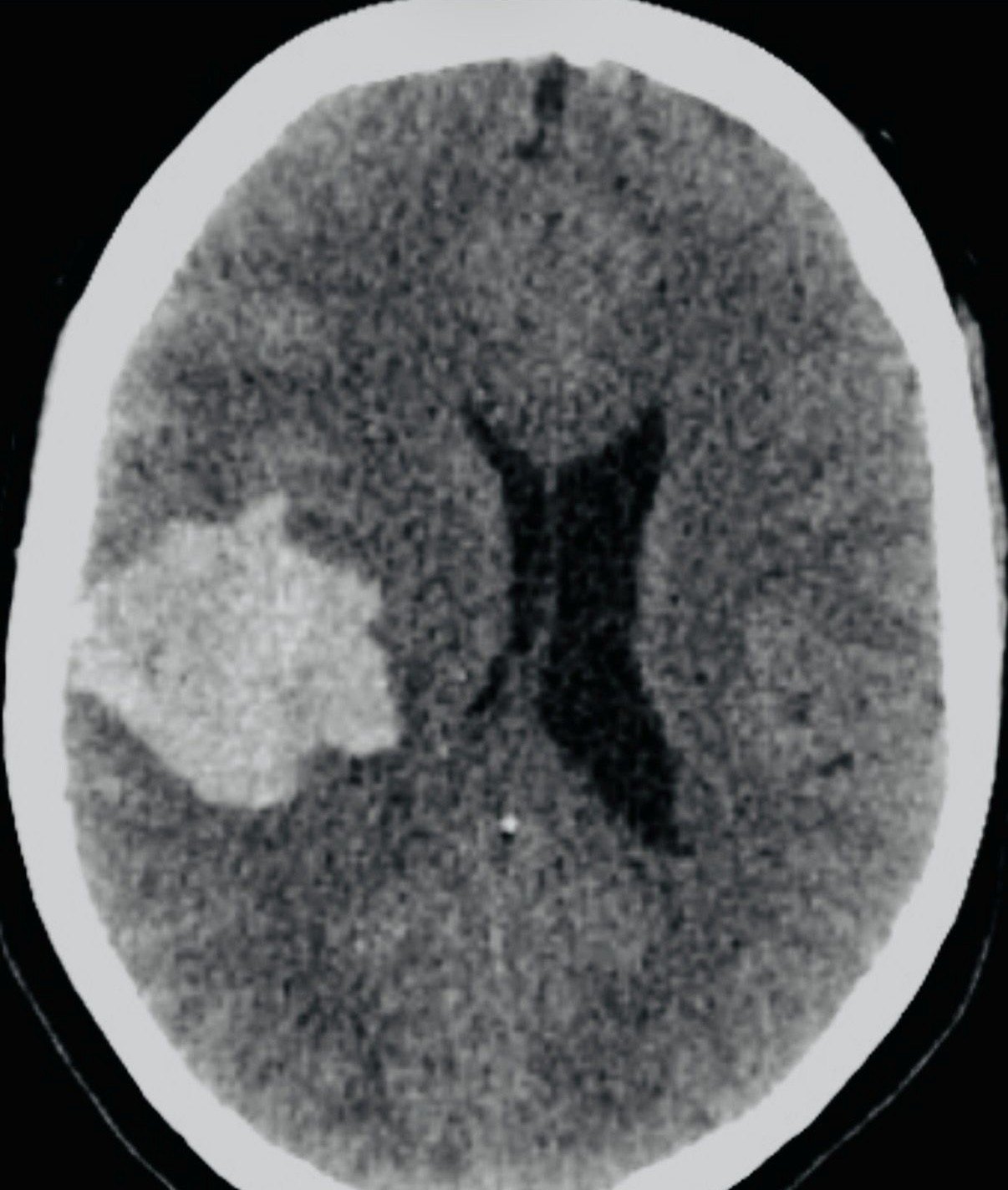
Stroke more often causes sudden face droop, arm weakness, speech trouble, vision loss, severe headache, or balance problems than simple fainting. Some brain bleeds or brainstem problems can present with collapse.
Clue: any sudden one-sided weakness, trouble speaking, severe headache, or new confusion is time-sensitive.
Collapse with focal deficits, severe thunderclap headache, depressed consciousness, anticoagulation, trauma, neck pain, posterior circulation signs, meningism, or persistent altered mental status should trigger neurologic emergency evaluation. Consider ischemic stroke, ICH, SAH, basilar occlusion, seizure mimic, infection, mass effect, and toxic-metabolic causes.
Low blood sugar can cause sweating, shaking, hunger, confusion, weakness, seizure, or collapse. It is especially important in people using insulin or sulfonylurea diabetes medicines.
Important: if someone is unconscious or cannot swallow safely, do not put food or drink in their mouth.
Check point-of-care glucose early. Consider hypoglycemia, DKA/HHS, hyponatremia, hyperkalemia, hypocalcemia, renal or hepatic failure, adrenal crisis, thyroid storm/myxedema, hypoxia, hypercapnia, and acid-base derangements. Medication reconciliation matters: insulin, sulfonylureas, beta blockers, alcohol, sedatives, opioids, and polypharmacy.
The brain needs enough blood pressure and oxygen. Major bleeding, severe dehydration, sepsis, allergic reactions, vomiting, diarrhea, heat illness, or internal bleeding can make blood pressure fall and cause collapse.
Clue: cold clammy skin, fast breathing, weakness, confusion, fever, rash, black stools, vomiting blood, or severe belly pain can be serious.
Evaluate for hypovolemic, distributive, cardiogenic, and obstructive shock. Search for hemorrhage, sepsis, anaphylaxis, adrenal crisis, PE, tamponade, tension pneumothorax, MI, dysrhythmia, GI bleed, ruptured ectopic pregnancy, ruptured AAA, and severe dehydration. Initial resuscitation and source control often precede definitive diagnosis.
Low oxygen can cause collapse. Causes include choking, severe asthma or COPD, pneumonia, overdose, carbon monoxide, a large blood clot in the lungs, or a collapsed lung.
Clue: blue lips, severe shortness of breath, wheezing, chest pain, or exposure to smoke or gas needs urgent care.
Assess SpO2 waveform quality, ventilation, airway obstruction, bronchospasm, aspiration, PE, pneumothorax, pneumonia, pulmonary edema, opioid or sedative toxidrome, carbon monoxide, methemoglobinemia, and neuromuscular weakness. Oxygen saturation can be misleading in CO poisoning.
Alcohol, sedatives, opioids, stimulants, blood pressure medicines, heart medicines, carbon monoxide, poisoning, head injury, heat stroke, and severe pain can all lead to collapse.
Pattern: scene clues matter: pill bottles, patches, fumes, heat exposure, fall risk, new medicines, or a witnessed injury.
Consider opioid, sedative-hypnotic, ethanol, stimulant, anticholinergic, cholinergic, salicylate, beta blocker, calcium channel blocker, digoxin, lithium, and CO exposures. Also assess trauma mechanism, occult head injury, cervical spine risk, hyperthermia, exertional heat stroke, rhabdomyolysis, and environmental exposure.
Safety
A short faint can still need medical review, but some collapse events are immediate emergencies. When in doubt, especially if the person is not waking normally, call emergency services.
The patient-facing symptoms below map to cardiac arrest, ACS, malignant arrhythmia, PE, stroke, seizure/status epilepticus, shock, hypoxemia, anaphylaxis, severe hypoglycemia, hyperthermia, intoxication, and trauma. First-pass actions: ABCs, CPR/AED if pulseless, glucose, ECG, SpO2, vitals including orthostatics when stable, temperature, trauma survey, and time-sensitive pathways.
Workup
Is the person awake? Are they breathing normally? Is there a pulse, severe bleeding, injury, or low oxygen? These checks decide how urgent the response is.
Blood sugar, blood pressure, oxygen, temperature, pulse, and an ECG can quickly reveal treatable problems.
What happened before, during, and after the collapse often gives the biggest clue, especially when the person cannot remember the event.
Blood tests, pregnancy testing, heart monitoring, brain imaging, chest imaging, toxicology, or specialist review may be needed depending on the pattern.
ABCs, CPR/AED when pulseless, hemorrhage control, oxygen/ventilation, IV/IO access, glucose, naloxone when indicated, seizure rescue therapy, cooling for heat stroke, and early escalation.
Vitals, orthostatics if stable, ECG, glucose, SpO2, temperature, CBC, CMP, Mg, troponin when indicated, lactate/VBG/ABG by acuity, pregnancy test, tox screen selectively, and medication review.
Structural heart disease, abnormal ECG, exertional or supine syncope, palpitations, family sudden death, persistent hypotension, dyspnea, anemia/bleeding, anticoagulation, focal neurologic deficit, and serious injury.
Telemetry, echo, CT/CTA, PE workup, EEG, infection evaluation, toxicology consultation, trauma imaging, obstetric pathway, endocrine testing, or admission decisions should follow the highest-risk phenotype.
Medical visuals




Languages
When this site is live, use the selector to open the page through Google Translate. The country presets are quick links for languages commonly needed in emergency care.
Sources